Introduction
Current trends in health reflect an important contemporary shift towards citizen engagement for health and prevention, as opposed to mere disease management.
However, broadcasting generic health messages (e.g. ‘do this, don’t do that’) has limited effects unless there is a convincing, easily perceived and personally customized body of evidence to back healthy choices.
OA risk calculators have been employed to help the public better perceive the risks and pitfalls of osteoarthritis.
Most prominent tools shown in the table below use risk estimations for OA derived from specific studies to create a digital tool that shows OA risks to the public.
OAPoI |
Osteoarthritis Policy Model, Brigham and Women’s Hospital, USA
https://pivot.bwh.harvard.edu/ongoing-projects/oapol
and
http://calculator.oarisk.org |
Initiated in 2006. A Monte Carlo computer simulation model to evaluate epidemiologic factors that affect knee OA. The model tracks every individual’s clinical course from the time of entry into the model to death, incorporating comorbidities, such as cancer, cardiovascular disease, and other musculoskeletal diseases, and traumatic knee injuries, such as anterior cruciate ligament and meniscal tears. The model then outputs population-level data, including our primary outcome measures: average quality-adjusted life expectancy and lifetime medical costs. |
TOARP |
Osteoarthritis Risk Prediction (TOARP), University of California. USA
Joseph GB et al. Tool for osteoarthritis risk prediction (TOARP) over 8 years using baseline clinical data, X-ray, and MRI: Data from the osteoarthritis initiative. J Magn Reson Imaging. 2018 Jun;47(6):1517-1526. doi: 10.1002/jmri.25892. |
Published in 2018 Osteoarthritis Initiative (http://www.oai.ucsf.edu) (11), a multi-center, longitudinal study of persons aged 45–79 years at enrollment, aimed at assessing biomarkers in OA including those derived from MR imaging. |
MSK |
Musculoskeletal Calculator, by Versus Arthritis and Imperial College London, UK
https://www.versusarthritis.org/policy/resources-for-policy-makers/musculoskeletal-calculator/msk-calculator-faq/ |
Uses data from UK specific clinical studies, such as (1) The English Longitudinal Study of Ageing (ELSA), (2) Health Survey for England (HSE) 2011, and (3) Clinical Practice Research Datalink (CPRD) to estimate prevalence of certain musculoskeletal disease including osteoarthritis. |
NOUS team created a new OA risk calculator that uses medical evidence from recent high evidence level medical publications.
The NOUS OA Risk Calculator is expandable and can include new risk evidence when this is published.
The tool is based on the CARRE health risk ontology and expands the CARRE health risk database
(CARRE is an EU FP7 ICT project, Contract No. 611140, https://www.carre-project.eu/).
Use the NOUS OA Risk Calculator here: https://nous.carre-project.eu/"
What data sources were used to calculate OA risks?
In order to identify high-level medical evidence of risk factors related to osteoarthritis,
2 team members (one student and one principal investigator) searched systematically in PubMed during September 2021.
PubMed (https://pubmed.ncbi.nlm.nih.gov/) is a biomedical citation database provided by the USA National Library of
Medicine and is considered one of the most comprehensive sources for biomedical literature search. The database provides
citation details for more than 33 million scientific publications in the biomedical sciences, including includes
guidelines and systematic reviews and meta-analyses produced by commonly accepted independent evidence bodies such as
Cochrane Collaboration
Risk factors identification methodology
Query |
(osteoarthritis risk) AND (meta-analysis) AND (last 5 years) |
Query as in PubMed |
(("osteoarthritis"[MeSH Terms] OR "osteoarthritis"[All Fields] OR "osteoarthritides"[All Fields]) AND ("risk"[MeSH Terms] OR "risk"[All Fields])) AND ((y_5[Filter]) AND (meta-analysis[Filter]))
|
Inclusion criteria |
meta-analyses reporting on risk for osteoarthritis
in human studies
in English language
reporting values for relative risk ratio (RR) or odds ratio (OR) or hazard ratio (HR)
reporting an acceptable level of evidence
|
Exclusion criteria |
studies considering their evidence level low or insufficient
animal studies
studies on risk or effectiveness of OA therapies
studies on genetic susceptibility for OA
studies on OA patients to identify risk for other disease
|
Risk factors identification results
Initially retrieved |
393 publications |
Retained after inclusion/exclusion criteria |
- Freiberg A, Bolm-Audorff U, Seidler A. The Risk of Knee Osteoarthritis in Professional Soccer Players. Dtsch Arztebl Int. 2021 Jan 29;118(4):49-55. doi: 10.3238/arztebl.m2021.0007
- Nie D, Yan G, Zhou W, Wang Z, Yu G, Liu D, Yuan N, Li H. Metabolic syndrome and the incidence of knee osteoarthritis: A meta-analysis of prospective cohort studies. PLoS One. 2020 Dec 23;15(12):e0243576. doi: 10.1371/journal.pone.0243576.
- Wang X, Perry TA, Arden N, Chen L, Parsons CM, Cooper C, Gates L, Hunter DJ. Occupational Risk in Knee Osteoarthritis: A Systematic Review and Meta-Analysis of Observational Studies. Arthritis Care Res (Hoboken). 2020 Sep;72(9):1213-1223. doi: 10.1002/acr.24333.
- Wang J, Dong J, Yang J, Wang Y, Liu J. Association between statin use and incidence or progression of osteoarthritis: meta-analysis of observational studies. Osteoarthritis Cartilage. 2020 Sep;28(9):1170-1179. doi: 10.1016/j.joca.2020.04.007.
- Poulsen E, Goncalves GH, Bricca A, Roos EM, Thorlund JB, Juhl CB. Knee osteoarthritis risk is increased 4-6 fold after knee injury - a systematic review and meta-analysis. Br J Sports Med. 2019 Dec;53(23):1454-1463. doi: 10.1136/bjsports-2018-100022.
- Sun Y, Nold A, Glitsch U, Bochmann F. Hip Osteoarthritis and Physical Workload: Influence of Study Quality on Risk Estimations-A Meta-Analysis of Epidemiological Findings. Int J Environ Res Public Health. 2019 Jan 24;16(3):322. doi: 10.3390/ijerph16030322.
- Zhang YM, Wang J, Liu XG. Association between hypertension and risk of knee osteoarthritis: A meta-analysis of observational studies. Medicine (Baltimore). 2017 Aug;96(32):e7584. doi: 10.1097/MD.0000000000007584.
- Kong L, Wang L, Meng F, Cao J, Shen Y. Association between smoking and risk of knee osteoarthritis: a systematic review and meta-analysis. Osteoarthritis Cartilage. 2017 Jun;25(6):809-816. doi: 10.1016/j.joca.2016.12.020
|
Results |
The above 8 publications produced:
7 risk factors
- knee injury --> knee osteoarthritis
- occupational exposure --> knee osteoarthritis
- occupational exposure --> hip osteoarthritis
- soccer playing --> knee osteoarthritis
- metabolic syndrome --> knee osteoarthritis
- hypertension --> knee osteoarthritis
- smoking --> knee osteoarthritis
27 different risk associations (OR= odds ratio, RR = relative risk)
- if knee injury = Anterior Cruciate Ligament injury
then knee osteoarthritis OR = 4.2 (2.2 to 8.0)
- if knee injury = Meniscal Injury
then knee osteoarthritis OR = 6.3 (3.8 to 10.5)
- if knee injury = (Meniscal Injury) AND (Anterior Cruciate Ligament Injury)
then knee osteoarthritis OR = 6.4 (4.9 to 8.3)
- if job = agriculture
then knee osteoarthritis OR = 1.64 (1.33 to 2.1)
- if job = metal worker
then knee osteoarthritis OR = 1.85 (1.25 to 2.76)
- if job = building and construction
then knee osteoarthritis OR = 1.63 (1.39 to 1.92)
- if job = floor and brick layer
then knee osteoarthritis OR = 2.51 (1.79 to 3.52)
- if job = carpenter
then knee osteoarthritis OR = 2.49 (1.66 to 3.74)
- if job = miner
then knee osteoarthritis OR = 1.47 (1.11 to 1.95)
- if job = cleaner
then knee osteoarthritis OR = 1.51 (1.14 to 2.01)
- if job = housework
then knee osteoarthritis OR = 1.93 (1.31 to 2.84)
- if job = service worker
then knee osteoarthritis OR = 1.79 (1.36 to 2.37)
- if job = craftsman
then knee osteoarthritis OR = 1.56 (1.17 to 2.09)
- if occupational activity = lifting
then knee osteoarthritis OR = 1.39 (1.22 to 1.59)
- if occupational activity = kneeling
then knee osteoarthritis OR = 1.29 (1.05 to 1.57)
- if occupational activity = standing
then knee osteoarthritis OR = 1.30 (1.09 to 1.53)
- if occupational activity = climbing
then knee osteoarthritis OR = 1.49 (1.20 to 1.86)
- if occupational activity = squatting
then knee osteoarthritis OR = 1.48 (1.21 to 1.81)
- if occupational activity = walking
then knee osteoarthritis OR = 1.23 (1.01 to 1.52)
- if occupational activity = sitting
then knee osteoarthritis OR = 0.77 (0.70 to 0.84) protective
- if occupational activity = lifting
then hip osteoarthritis OR = 2.00 (1.34 to 2.99)
- if job = agriculture
then hip osteoarthritis OR = 4.74 (2.84 to 7.89)
- if (sex=male AND soccer playing status = professional)
then knee osteoarthritis OR = 2.25 (1.41 to 3.61)
- if (sex = female AND metabolic syndrome diagnosis = yes)
then knee osteoarthritis RR = 1.23 (1.03 to 1.47)
- if hypertension diagnosis = yes
then knee osteoarthritis OR = 1.49 (1.26 to 1.77)
- if (sex = male AND smoking status = smoker)
then knee osteoarthritis OR = 0.69 (0.58 to 0.80) protective
- if (sex = female AND smoking status = smoker)
then knee osteoarthritis OR = 0.89 (0.77 to 1.02) protective
- if statin administration = yes
then osteoarthritis OR = 1.01 (0.96 to 1.05) no association
|
Limitations |
only meta-analyses were included, however, a wider search might reveal individual cohort studies of high quality
search limited only to the last five years
search limited only to PubMed and primary search results
included only papers reporting risk for OA, future work should expand to include any risk associated with OA and related conditions, diseases and comorbidities
|
The Software
CARRE risk factor ontology – conceptual model (CARRE D.2.2, 2014 https://www.carre-project.eu/project-info/deliverables-2/
and available via the NCBO BioPortal https://bioportal.bioontology.org/ontologies/CARRE).
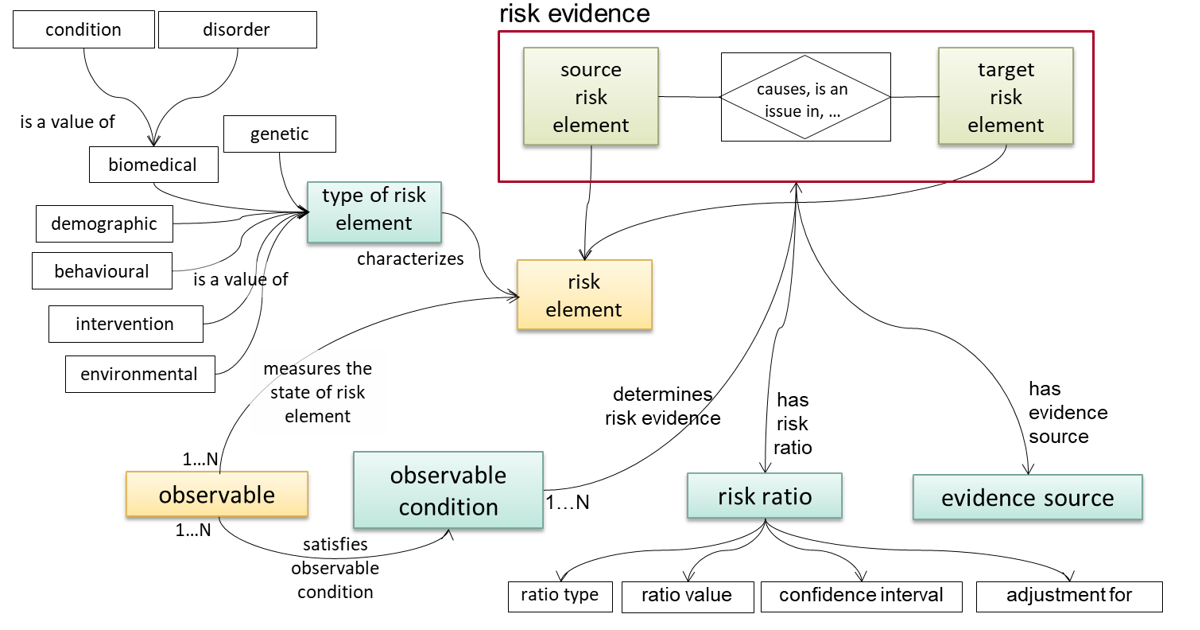
Figure 1: CARRE risk factor ontology – conceptual model.
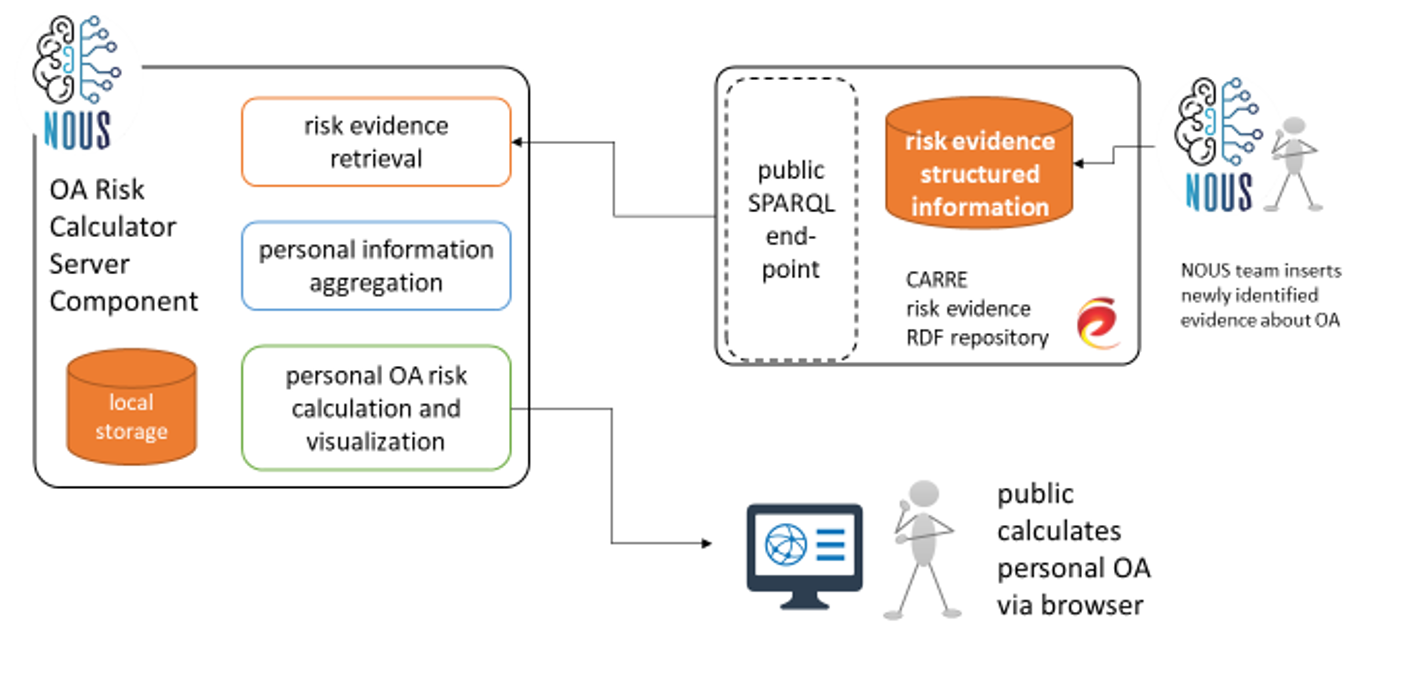
Figure 2: System high level architecture.